

A chiropractor in Denver showed me their denial report last month. Thirty-eight percent of their claims for spinal manipulation were getting kicked back. Not because the treatment wasn't necessary. Not because the patient didn't have coverage. The denials came down to three missing words in their documentation: "audible joint release."
This happens constantly with chiropractic CPT codes. You can deliver perfect care, transform a patient's quality of life, and still lose thousands in revenue because your documentation didn't include the magic phrases that insurance reviewers scan for.
After analyzing denial patterns across dozens of practices, certain mistakes show up constantly. The same CPT codes get misused. The same documentation gaps trigger rejections. Clinics keep submitting appeals without the specific language that actually gets denials overturned.
The 98940 vs 98941 Documentation Trap
Most chiropractors know 98940 covers one to two spinal regions while 98941 covers three to four. What kills reimbursement is how you document those regions. Insurance companies don't count "low back" as a region. They want specifics: lumbar spine (L1-L5), sacrum, pelvis. Each documented separately. A typical denied claim reads "adjusted lower back and mid back" when it should specify "L3-L5, T6-T8, left sacroiliac joint."
Documentation requirements for 98941 (three to four regions):
-
Specific vertebral levels adjusted (not just "cervical" or "thoracic")
-
Side designation when applicable (left SI joint, right rib)
-
Type of adjustment performed (diversified, drop table, activator)
-
Patient positioning during adjustment
-
Line of drive or contact point
Sample documentation that works:
"Patient positioned prone. Diversified adjustment performed:
-
C2-C3 posterior to anterior, bilateral
-
T4-T6 posterior to anterior with right lateral flexion
-
L4-L5 posterior to anterior
-
Left sacroiliac joint, posterior superior to anterior inferior
Audible release noted at T4 and L4. Patient tolerated procedure well."
Bill 98941 with vague documentation like "full spine adjustment"? You're asking for a denial.
Extraspinal CMT: Why 98943 Gets Rejected
Code 98943 covers extraspinal regions — ribs, extremities, TMJ. The denial rate on this code runs around 45% for practices that don't document the medical necessity properly.
Never miss another patient appointment.
Spinesly helps you schedule, confirm, and manage every patient visit efficiently.
- Unified appointment management
- Automated patient reminders
- Staff and resource scheduling
No credit card required
The problem: you can't just note "adjusted right shoulder." Insurance wants to know why chiropractic manipulation was medically necessary versus sending them to physical therapy.
Documentation that prevents 98943 denials:
"Right glenohumeral joint restriction identified through motion palpation. Passive range of motion limited to 110 degrees flexion (normal 180). Joint dysfunction directly related to compensatory patterns from C5-C6 subluxation complex previously documented. Chiropractic manipulative therapy indicated to restore joint mechanics as component of spinal kinetic chain. Manipulation performed: Right glenohumeral joint, anterior to posterior glide with circumduction. Post-adjustment ROM improved to 145 degrees flexion."
Notice how this ties the extremity work back to the spine? That's what gets it covered. Pure extremity work without spinal involvement often gets denied under chiropractic benefits.
The Modality Confusion with 97140
Manual therapy (97140) causes more coding headaches than almost any other code in chiropractic practices. The confusion: thinking it covers any hands-on soft tissue work.
Insurance companies audit 97140 claims looking for these specific techniques:
-
Myofascial release
-
Trigger point therapy
-
Manual lymphatic drainage
-
Manual traction
-
Soft tissue mobilization
What doesn't qualify: general massage, stretching a patient can do themselves, or passive modalities like ultrasound.
97140 documentation that survives audit:
"15 minutes manual therapy to right upper trapezius and levator scapulae. Technique: myofascial release using cross-fiber friction and pin-and-stretch methodology. Identified trigger point at superior angle of scapula, applied sustained pressure 30-60 seconds until release palpated. Post-treatment: improved cervical rotation from 45 to 65 degrees right."
Time matters here. Bill one unit (15 minutes) and document exactly 15 minutes. Bill two units without documenting 30 minutes of hands-on time? Automatic denial.
X-Ray Documentation Requirements
The days of routine x-rays on every new patient ended years ago, but practices still submit 72040 (cervical spine x-ray) without proper medical necessity documentation.
What triggers x-ray denials:
-
"New patient evaluation" as the only reason
-
No red flags documented
-
Missing clinical decision rules
-
Ordering full spine series without specific indications
X-ray documentation that gets approved:
"72040 cervical spine series ordered based on:
-
Patient reports trauma
motor vehicle accident 6 days ago
-
Canadian C-Spine Rule positive
age over 65, paresthesias in bilateral upper extremities
-
Physical exam
limited ROM less than 45 degrees rotation bilaterally
-
Suspected pathology requiring ruling out fracture/instability before manipulation
You're showing clinical reasoning, not routine screening.
Therapeutic Exercise Coding Disasters
97110 (therapeutic exercise) seems straightforward until you realize insurance companies expect detailed progression notes.
A denied 97110 claim usually looks like: "Patient performed exercises, 15 minutes."
What passes review:
"97110 - Therapeutic exercises, 15 minutes
-
Dead bug progression
3 sets x 8 reps, added 2-pound ankle weights (increase from bodyweight last visit)
-
Bird dog holds
3 sets x 15-second holds each side, progressed from quadruped to standing position
-
Lumbar stabilization on therapy ball
2 sets x 12 reps, reduced base of support from feet 12 inches apart to 6 inches
Patient demonstrated improved motor control, reduced compensatory patterns. Home program updated with progressions."
The key: show progression. Same exercises week after week? That's maintenance, not therapeutic. Insurance stops paying.
Evaluation Code Selection Mistakes
New patient evaluations generate denials when practices automatically bill 99204 (moderate to high complexity) for everyone.
Insurance reviewers check if your documentation supports the complexity level:
99203 (low to moderate complexity) requires:
-
Limited number of diagnoses
-
Low risk of complications
-
Straightforward data review
99204 (moderate to high complexity) needs:
-
Multiple diagnoses or complex presentation
-
Moderate risk factors
-
Extensive data review or ordering of tests
Documentation that supports 99204:
"45-minute evaluation completed. History reveals chronic low back pain with radicular symptoms, failed conservative care including 12 PT sessions, previous epidural injection. Review of outside MRI report shows L4-L5 disc herniation with nerve root compression. Prescription medications reviewed: gabapentin, cyclobenzaprine. Physical examination: comprehensive musculoskeletal and neurological testing including DTRs, dermatomal sensation, myotomal strength testing, straight leg raise positive at 35 degrees right. Assessment: Complex presentation requiring coordination with primary care, possible surgical consultation if conservative care fails."
Bill 99204 for simple mechanical back pain without complications? Expect a downgrade to 99203 and a refund request.
The Re-Evaluation Timing Problem
97161-97163 (physical therapy evaluation codes that some chiropractors use) and chiropractic-specific re-evaluation coding create confusion around timing.
Practices bill re-evaluations every 30 days thinking that's standard. Insurance companies look for documented changes in condition that justify re-assessment.
Re-evaluation triggers that get paid:
-
Plateau in progress for 2+ weeks
-
New symptoms or injury
-
Significant functional change
-
Pre/post intensive treatment period
-
Return after discharge
Documentation that justifies re-evaluation:
"Re-evaluation performed due to patient reporting new radiating symptoms to left leg beginning 5 days ago, not present at initial evaluation. Complete reassessment indicates:
-
Original cervical complaint
70% improved
-
New finding
Positive slump test left, absent at initial eval
-
Modified treatment plan
Adding McKenzie extension protocol, reducing cervical focus
-
Referral for lumbar MRI to rule out disc pathology
Without documenting why you're re-evaluating beyond "it's been 30 days," expect denials.
Maintenance Care Documentation Landmines
Practices hemorrhage money billing active treatment codes for maintenance care.
Words that trigger maintenance flags:
-
"Preventive"
-
"Wellness"
-
"Monthly adjustment"
-
"Maintaining correction"
-
"Prevent re-occurrence"
The patient might need ongoing care, but insurance reads those words and immediately denies.
Instead, document ongoing medical necessity:
"Patient continues to demonstrate functional deficits:
-
Sits maximum 45 minutes before pain onset (job requires 8-hour sitting)
-
Unable to lift 25 pounds without guarding (childcare duties require 35-pound lifting)
-
Pain increases to 6/10 with prolonged standing at work
-
Objective
Reduced lumbar flexion 60 degrees (normal 90), positive Kemp's test right
Treatment today focused on improving functional capacity for work duties."
That same patient might be coming monthly, but you're documenting active problems and functional limitations, not maintenance.
Common Appeal Language That Actually Works
When denials hit, generic appeals fail. Insurance companies want specific clinical reasoning.
For medical necessity denials:
"Regarding denial for date of service [DATE], CPT 98941:
-
Objective findings
Restricted intersegmental motion T6-T9 with palpable muscle spasm
-
Functional limitation
Patient unable to perform job duties (package delivery) due to thoracic pain with lifting
-
Active treatment plan
2x weekly for 3 weeks with specific goal of returning to full work duties
-
Progress documented
Pain reduced from 7/10 to 4/10, lifting capacity increased from 15 to 25 pounds
This represents active treatment for diagnosed subluxation with functional deficits, not maintenance. Request reversal of denial and payment per contracted rates."
For coding denials:
"CPT 98943 denied as 'not covered service'
-
The extremity manipulation was medically necessary component of spinal treatment:
-
- Primary diagnosis
Cervical subluxation C5-C6
-
- Secondary finding
Compensatory shoulder dysfunction limiting cervical rotation
-
- Manipulation of glenohumeral joint required to achieve full cervical restoration
-
- Post-treatment
Cervical rotation improved from 45 to 70 degrees
This meets criteria for 98943 as extraspinal manipulation directly related to spinal condition. Supporting documentation attached."
The Electronic Documentation Advantage
Manual documentation kills efficiency and creates denial risks. You're typing the same phrases repeatedly, missing key elements when rushed, and creating inconsistent records.
AI-powered operational platforms now generate compliant documentation while you treat. The software captures required elements for each CPT code — specific vertebral levels, technique descriptors, medical necessity language — without you thinking about it.
A practice in Phoenix integrated AI-assisted documentation and dropped their denial rate from 31% to around 8% in four months. The system prompts for missing elements specific to each code billed. No more forgetting to document "audible release" for 98940 or progression notes for 97110.
The automation also builds a library of successful appeal language. When denials occur, it pulls previous successful appeals for similar scenarios and generates appeals that actually get paid.
Documentation Shortcuts You Can't Take
Certain shortcuts guarantee denials:
| Shortcut | Explanation |
|---|---|
| Cloned notes: | Copy-pasting creates identical documentation across visits. Reviewers spot this immediately. Even with templates, each note needs unique findings and progress indicators. |
| Missing pain scales: | Not documenting pain levels pre and post-treatment makes it impossible to show improvement. "Patient feels better" doesn't cut it. "Pain decreased from 6/10 pre-treatment to 3/10 post-treatment" does. |
| Vague body regions: | "Mid-back" doesn't specify thoracic levels. "Neck" doesn't indicate cervical segments. Get specific or get denied. |
| Absent functional goals: | "Reduce pain" isn't a functional goal. "Return to playing tennis 3x weekly without limitation" is. Insurance wants to know when active care ends. |
| Generic treatment descriptions: | "Adjusted spine" tells reviewers nothing. "Diversified manipulation C5-C6, posterior to anterior, supine position" tells them everything. |
Get specific or get denied.
Building Your Denial Prevention System
Practices with lowest denial rates don't rely on memory. They build systematic approaches:
Create CPT-specific documentation templates that include all required elements. Not generic SOAP notes — templates designed for each code you bill frequently.
Train staff on denial patterns. Your front desk should know that scheduling "maintenance adjustments" triggers denials before claims get submitted. Use terms like "follow-up evaluation" or "re-assessment for ongoing symptoms."
Review denials weekly, not monthly. Patterns emerge quickly. If 98942 keeps getting denied, your documentation for five or more regions needs work. Fix it before submitting more claims with the same problem.
Track denial rates by code, by payer, by provider. One associate might document perfectly while another triggers constant denials.
Stop treating documentation as an afterthought. The three minutes spent adding specific details saves hours of appeals and thousands in lost revenue. Every adjustment you make deserves documentation that ensures you get paid for it.
Here's a simple workflow for a denial prevention system.
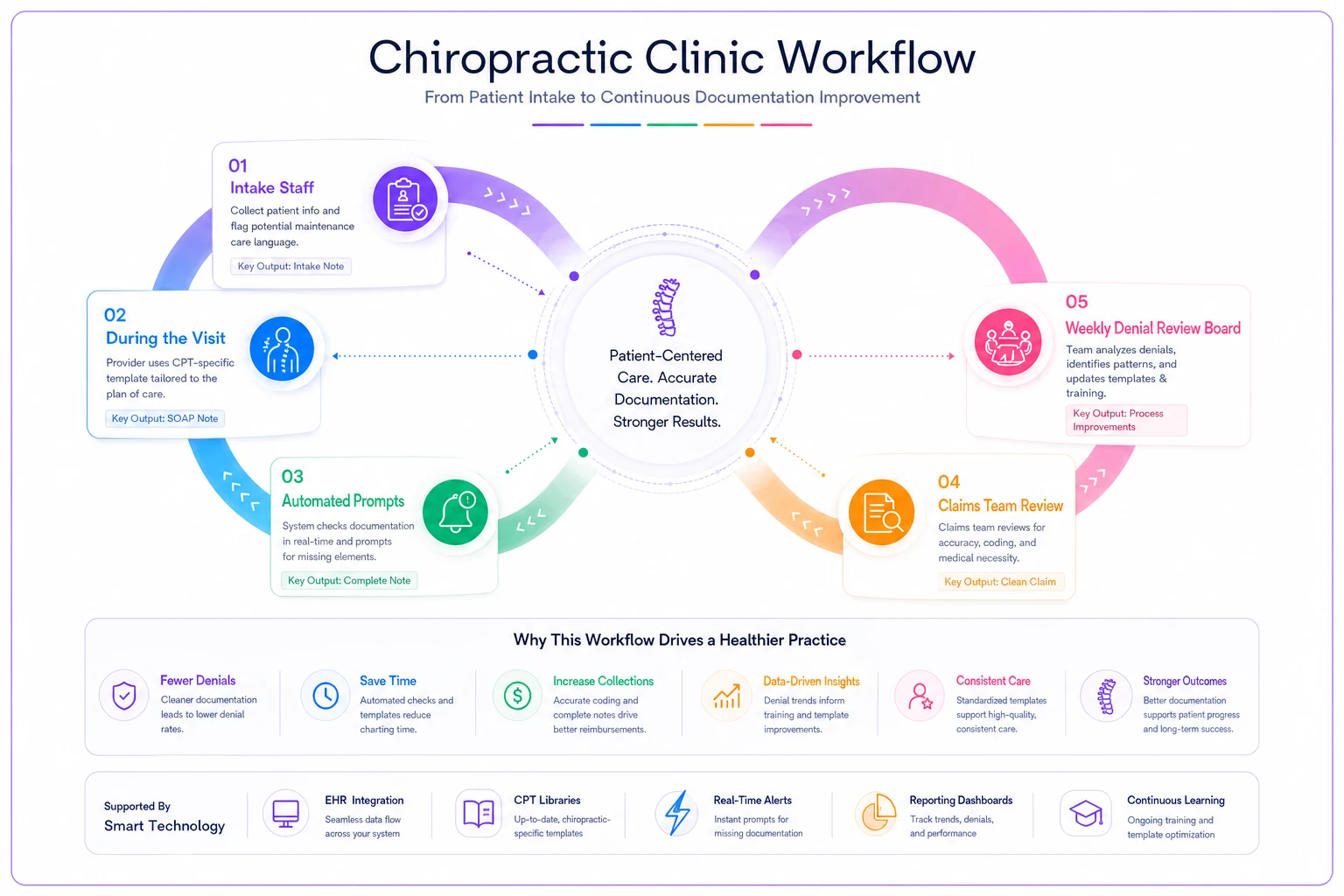
The difference between practices losing 30% to denials and those under 10% isn't the quality of care. It's the quality of documentation.
Run a weekly denial report filtered by CPT and provider so you can correct documentation patterns before filing new claims.
Practices using AI-powered platforms to ensure documentation completeness while reducing administrative burden maintain healthy revenue cycles without burning out their providers on paperwork.
Your documentation tells the story of why each service was necessary, what specifically was done, and what improvement occurred. Tell that story clearly, with the right details, and denials become rare exceptions instead of daily frustrations.
Your documentation tells the story of why each service was necessary, what specifically was done, and what improvement occurred. Tell that story clearly, with the right details, and denials become rare exceptions instead of daily frustrations.
Ready to streamline your chiropractic clinic operations?
Join 1,200+ clinics using Spinesly to save time, reduce scheduling errors, and improve patient care experiences.