

Three months ago, a chiropractor in Georgia called me about their collections dropping from 94% to 71% over six months. Their billing company blamed insurance changes. Front desk pointed to unclear documentation requirements. The associate doctors figured it was coding complexity.
They were all looking at symptoms, not the disease.
The real issue? Their revenue cycle was held together with digital duct tape. One insurance requirement change, one sick staff member, one busy week—and money started hemorrhaging through preventable cracks.
This Georgia clinic isn't unique. Building operational software for chiropractic practices, you see the same pattern everywhere: clinics treat revenue cycle management like it's about submitting clean claims when it's actually about building a machine where every piece feeds perfectly into the next.
The hidden architecture of chiropractic revenue cycle management
Most chiropractors think RCM starts at claim submission. That's like thinking your car starts at the muffler. Revenue cycle begins when someone considers booking an appointment—every touchpoint after that either strengthens or destroys your ability to collect.
The full operational flow in a well-running clinic:
Pre-appointment phase:
-
Insurance verification triggers when appointment books
-
Benefits check includes visit limits, authorization requirements, deductible status
-
Documentation requirements get flagged for specific payers
-
Patient financial responsibility gets calculated and communicated upfront
Service delivery phase:
-
Exam documentation captures medical necessity from first contact
-
Treatment notes align with payer-specific requirements
-
Coding rules apply based on diagnosis and treatment combination
-
Modifier requirements get checked against payer contracts
Post-service phase:
-
Claims generate with pre-validated data
-
Submission timing follows payer preferences
-
Denial patterns trigger immediate corrections
-
Payment posting feeds back into eligibility tracking
Clinics collecting 95%+ of billed charges aren't just better at billing. They've connected these phases into one flow where Tuesday's eligibility check automatically adjusts Thursday's documentation requirements.
Why traditional billing approaches break at scale
When you're seeing 40 patients weekly, you can probably remember that Blue Cross requires progress notes every 12 visits and Aetna wants re-exams every 30 days. Your brain becomes the system. Around 80 weekly visits though, human memory stops being reliable infrastructure.
Never miss another patient appointment.
Spinesly helps you schedule, confirm, and manage every patient visit efficiently.
- Unified appointment management
- Automated patient reminders
- Staff and resource scheduling
No credit card required
Phoenix clinic learned this painfully. They grew from one doctor to three over 18 months. Collection rate dropped 22% during that growth. Not because new doctors documented poorly—because their manual tracking couldn't handle triple the information flow.
Their "eligibility verification" was a weekly-updated spreadsheet. Authorization tracking lived on monitor sticky notes. Documentation standards varied based on who trained which staff member. Every new patient, insurance plan, team member added another potential failure point.
The breaking point: hiring a fourth front desk person. She'd worked at a medical clinic, didn't know chiropractic-specific modifiers. Over six weeks, she scheduled 180 appointments. Nearly half got denied for coding issues that proper eligibility gating would have caught. Lost roughly $28,000 in revenue they never recovered.
Scheduling as your first line of revenue defense
Your scheduler is either protecting revenue or generating denials. No middle ground. Most clinics treat scheduling like a calendar problem when it's complex eligibility and workflow orchestration.
What actually needs to happen when someone books:
Insurance verification runs—not just active/inactive, but remaining benefits, visit limits, authorization requirements, excluded services. That information routes to the right people. Front desk needs copay and deductible info. Treating doctor needs documentation requirements. Billing team needs timely filing limits.
California clinic was losing $4,100 monthly from scheduling patients with exhausted benefits. Their scheduler showed "availability" with zero connection to eligibility data. Patients completed entire treatment plans before anyone realized insurance stopped paying eight visits ago.
The fix was operational gates in scheduling flow:
-
New patient books online → automatic eligibility check triggers
-
System identifies Medicare Advantage plan → flags additional authorization requirements
-
Front desk gets task to obtain authorization before visit
-
Patient receives automated message about potential costs
-
Documentation requirements auto-populate in EHR based on payer rules
Route eligibility results to the right people automatically so front desk, treating doctors, and billing teams each get the specific information they need.
Collection rate on new patients jumped from 76% to 91% within two months. Not better billing—better operational gates at patient journey start.
The documentation cascade that determines payment
Chiropractic documentation isn't just clinical notes—it's creating an evidence chain that satisfies aggressive payer audits. Every insurance company has different requirements. Missing one element tanks the entire claim.
The most expensive documentation mistakes happen in gaps between:
-
Initial exam and treatment plan connection
-
Progress notes and medical necessity evolution
-
Re-exam findings and continued care justification
-
Daily notes and diagnosis code alignment
Florida practice with two locations discovered this after BCBS audit recovered $47,000. Not fraudulent billing or bad coding—they hadn't connected documentation dots clearly enough. Initial exams were thorough. Daily notes were complete. But nowhere did they explicitly link ongoing treatment to measurable functional improvement.
Proper documentation flow:
| Documentation Stage | Required Elements | Common Failure Points | Revenue Impact |
|---|---|---|---|
| Initial Exam | Pain scales, functional assessments, diagnosis rationale | Missing objective findings | Claims denied from visit 1 |
| Treatment Plan | Frequency, duration, specific goals | Vague improvement targets | Authorizations rejected |
| Progress Notes | Measurable changes, plan modifications | No link to initial findings | Payment stopped mid-treatment |
| Daily Notes | Service specifics, response to care | Missing medical necessity | Individual visits denied |
| Re-exams | Comparative analysis, continued care justification | No measurable progress shown | Future visits unauthorized |
Clinics maintaining 95%+ clean claim rates don't write better notes—they build documentation checkpoints ensuring every required element gets captured before claim generation.
Why coding rules need operational enforcement, not memorization
Chiropractic coding is complex because you're coding the relationship between diagnosis, treatment, and medical necessity across multiple visits. Get one modifier wrong on visit three, and visits four through twelve might all get denied retroactively.
The problem isn't that coding is hard. Most clinics try enforcing coding rules through training instead of operational systems. Your team shouldn't need to remember that 98941 requires documentation of four spinal regions—your system should prevent using that code without proper documentation already in place.
Texas practice learned this after their new billing person accidentally used AT modifiers on maintenance care for three months. Cost them $31,000 in recoupments. They'd trained her extensively. She had coding charts on her wall. Still made the mistake because nothing in their flow prevented it.
Smart clinics build coding rules into operational software:
-
Diagnosis codes limit available procedure codes
-
Documentation completion gates code selection
-
Payer-specific rules override general coding
-
Historical patterns flag unusual combinations
-
Modifier requirements auto-populate based on visit number
This isn't replacing human judgment—it's creating operational guardrails that prevent expensive mistakes when someone's having an off day or training new staff.
The follow-up sequence that separates 72% from 95% collection rates
Most clinics think denied claims are a billing problem. They're actually an operational intelligence problem. Every denial contains information about what your upstream processes missed. Clinics stuck at 72% treat denials as one-off issues. Those hitting 95% treat them as system feedback.
Follow-up sequence that works:
Immediate response layer (0-48 hours): Denial hits → categorization by type → automated initial response based on denial code → documentation pulled if needed → resubmission or appeal initiated
Pattern recognition layer (weekly): Denial trends analyzed → root causes identified → operational adjustments made → staff notifications sent → process updates documented
Prevention layer (ongoing): Historical denial patterns inform future checks → eligibility verification adjusts for problem payers → documentation requirements update based on audit results → coding rules evolve with payer changes
Illinois clinic reduced denial rate from 18% to 6% not by working denials harder, but by building this feedback loop into operations. Every denial automatically triggered review of original scheduling, eligibility, documentation, and coding decisions. They discovered 40% of denials traced back to scheduling issues—patients booked without proper authorization or beyond benefit limits.
Building your minimum viable RCM operation
Trying to fix everything at once fixes nothing effectively. Start with highest-impact operational improvements for immediate revenue recovery:
Week 1-2: Fix your eligibility gating Connect insurance verification to scheduling system. Even if manual initially, no patient gets scheduled without benefits confirmed. This typically recovers 8-12% of lost revenue.
Week 3-4: Standardize documentation checkpoints Create hard stops in workflow—treatment notes can't be signed without required elements, claims can't generate without complete documentation. Pick your three biggest payers and nail their requirements first.
Week 5-6: Implement coding guardrails Build simple matrix of allowed diagnosis/procedure combinations. Make it impossible to submit claims with known problematic code pairs. Focus on most-used codes first.
Week 7-8: Activate denial feedback loops Every denial gets categorized and traced to origin point. Weekly reviews identify patterns. Monthly operational adjustments prevent future occurrences.
A simple visual to follow the week-by-week progression.
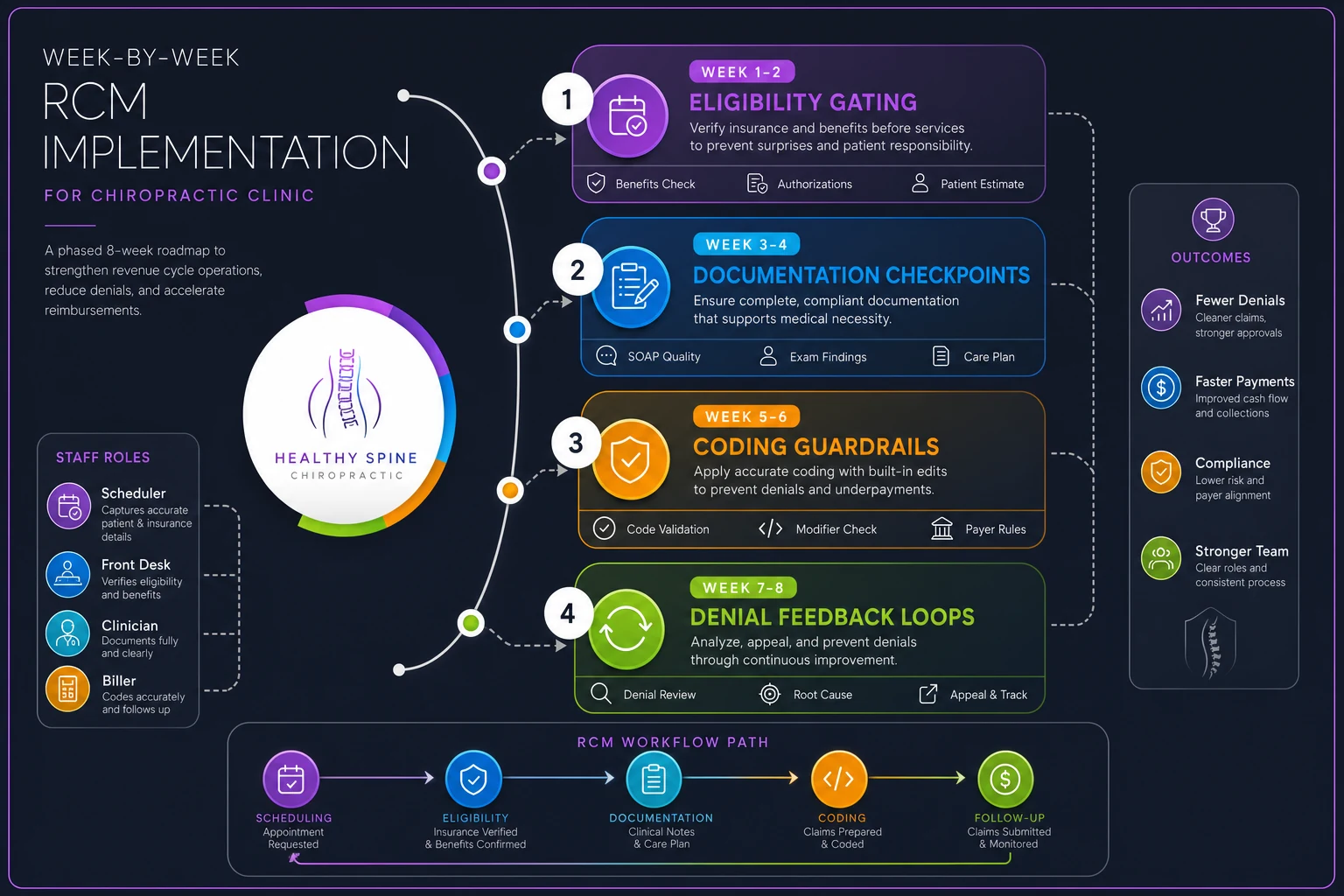
This progression takes you from reactive to proactive revenue cycle management. You're no longer chasing payments—you're preventing losses before they happen.
When small clinics actually outperform large ones
Being small is only a disadvantage if you're trying to operate like you're large. Small clinics can pivot faster, implement changes immediately, and maintain direct accountability that large practices struggle with.
Solo practitioner in Oregon consistently hits 97% collection rates—better than practices ten times their size. Their approach? Build entire operation around preventing problems rather than fixing them:
-
Every new patient gets financial consultation before treatment starts
-
Documentation requirements display on screen during exams
-
Coding suggestions appear based on documented findings
-
Claim generation waits for documentation completeness
-
Denial patterns immediately update future workflows
They're not working harder than larger clinics. They've built better operational connections between each revenue cycle part.
The technology layer that multiplies human effort
Throwing software at broken processes just digitizes chaos. But adding AI-powered operational software to solid RCM foundation multiplies your team's effectiveness exponentially.
Modern operational platforms can:
-
Run eligibility checks across multiple payers simultaneously
-
Flag documentation gaps before claim submission
-
Suggest coding based on documentation patterns
-
Predict denial probability before submission
-
Automate follow-up sequences based on payer preferences
-
Track collection patterns to identify process breakdowns
The key is "operational"—these tools work because they understand full workflow, not isolated tasks. They connect scheduling to eligibility to documentation to coding to follow-up in one continuous flow.
Arizona practice implemented connected operational software after struggling with 70% collection rates despite two full-time billing people. Within four months, they hit 93% collections with same team. Software didn't replace human judgment—it eliminated manual work preventing their team from exercising that judgment effectively.
Measuring what matters: operational metrics vs vanity numbers
Days in AR, clean claim rates, denial percentages—important, but trailing indicators. They tell you what already went wrong. Metrics that actually drive revenue improvement are operational:
-
Scheduling quality score
Percentage of appointments booked with complete eligibility verification
-
Documentation completion rate
Percentage of visits with all required elements captured before claim generation
-
First-pass resolution rate
Percentage of claims that pay without follow-up needed
-
Denial prevention rate
Percentage of potential denials caught before submission
-
Revenue capture velocity
Average time from service to payment posting
Track these weekly, not monthly. They show exactly where your revenue cycle is breaking before it shows up in your bank account.
The path forward: from reactive billing to proactive operations
Your chiropractic revenue cycle management isn't about managing revenue—it's about building operational excellence that makes revenue collection inevitable. Every patient interaction, documentation decision, coding choice either strengthens or weakens that inevitability.
Clinics thriving in today's complex reimbursement environment haven't figured out secret billing tricks. They've recognized that RCM is an operational challenge requiring operational solutions. They've connected scheduling, eligibility, documentation, coding, and follow-up into one coherent system where information flows seamlessly and problems get prevented rather than fixed.
Start with basics: gate scheduling with eligibility checks, standardize documentation requirements, enforce coding rules systematically, and build feedback loops from every denial. As foundations solidify, layer in automation and AI-powered tools that multiply team effectiveness.
The difference between 70% and 95% collection rates isn't billing expertise—it's operational discipline. Build the system, trust the process, and watch revenue recovery transform from constant struggle to predictable outcome.
Ready to streamline your chiropractic clinic operations?
Join 1,200+ clinics using Spinesly to save time, reduce scheduling errors, and improve patient care experiences.