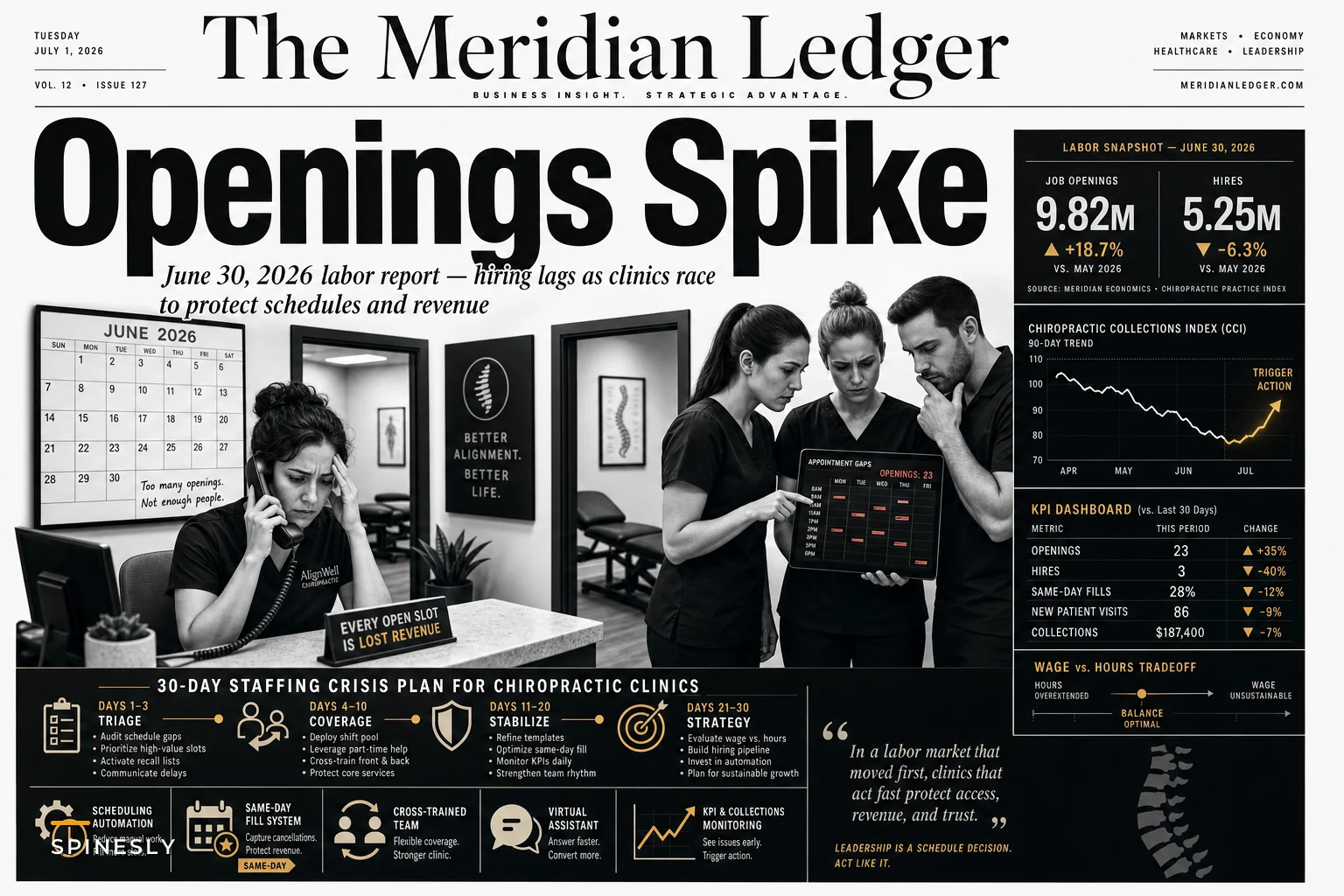

Job openings hit a two-year high in May while actual hiring stayed flat, according to Reuters. More open positions, fewer people taking them—and your front desk coordinator who just gave notice is about to be a lot harder to replace than you think.
This isn't just another hiring headache. When openings rise and hiring stalls simultaneously, you get wage pressure, longer vacancy windows, and staff who know they have leverage. For clinics running 3-5 core people, losing even one creates immediate operational chaos.
The timing is rough. Summer brings vacation gaps, back-to-school sports physicals, and the quarterly insurance verification crunch. Meanwhile, your existing team is getting recruited by competitors offering signing bonuses and remote options you can't realistically match.
Why standard clinic staffing strategies break down in this environment
Most chiropractic clinics approach staffing the same way they always have: post on Indeed, interview whoever applies, hope for the best. That playbook assumes a functional labor market where qualified candidates actually show up.
What's happening instead? Clinics are seeing dramatically fewer applications than two or three years ago. The ones that do come through often ghost interviews or accept offers and no-show on day one. Even successful hires are getting poached within 90 days by larger healthcare systems with better benefits.
The damage compounds fast. Your office manager covers front desk gaps, so insurance verifications pile up. Your lead CA handles scheduling overflow, so recall campaigns stop. Everyone's doing someone else's job, nobody's doing their actual job well, and patient experience suffers while burnout accelerates.
One three-location practice in Arizona lost around $47,000 in monthly revenue—not from fewer patients, but from scheduling falling apart after their coordinator left. They had patients wanting appointments and doctors with open slots, but nobody connecting the two effectively. Chair utilization dropped from 78% to 51% in about six weeks.
The scheduling cascade that kills revenue
When staffing gaps hit, scheduling is the first thing that unravels. Not because appointments stop coming in. But because managing provider preferences, patient requests, insurance requirements, and operational constraints is genuinely complicated—and it falls apart without experienced staff running it.
Never miss another patient appointment.
Spinesly helps you schedule, confirm, and manage every patient visit efficiently.
- Unified appointment management
- Automated patient reminders
- Staff and resource scheduling
No credit card required
A typical scheduling interaction actually involves:
-
Verifying insurance eligibility and visit limits
-
Checking provider availability against patient preferences
-
Identifying potential care plan conflicts
-
Flagging expired authorizations
-
Coordinating with the therapy schedule if needed
-
Booking the right visit duration based on visit type
New or temporary staff miss these details. They book new patients during lunch, schedule Medicare patients with non-participating providers, or stack back-to-back complex cases that destroy provider productivity. Each mistake costs somewhere in the $120-180 range in lost revenue opportunity.
The real problem is these errors don't surface immediately. You discover them three weeks later when patients complain about wait times, claims get denied, or your providers are exhausted. By then you've already lost thousands and damaged multiple patient relationships.
Building contingency systems before crisis hits
Some clinics have stopped chasing the perfect full-time hire and started building flexible coverage systems that assume constant staffing volatility. It's a different mental model, but it holds up better in practice.
Start with role fragmentation. Instead of hiring one person to handle all front desk duties, split responsibilities into discrete, trainable chunks:
Core scheduling tasks (can be remote):
-
Appointment booking
-
Reminder calls
-
Waitlist management
-
Basic eligibility checks
In-office requirements (must be on-site):
-
Patient check-in
-
Payment collection
-
Forms assistance
-
Provider support
This separation opens up different labor pools. Remote scheduling can pull from virtual assistants, stay-at-home parents, or shared resources across multiple locations. In-office tasks can use part-time staff, college students, or cross-trained clinical assistants who already know the patients.
A clinic group in Ohio tried this after losing three front desk staff in two months. They hired two remote schedulers at $18/hour to handle all phone and booking tasks, then staffed the physical desk with rotating clinical assistants. Result: 30% lower staffing costs, zero scheduling gaps during transition.
The cross-training matrix that actually works
Every clinic claims to cross-train. Most just show people where things are located and call it done. Real cross-training means building measurable competency in specific tasks that can be activated during coverage gaps—not general familiarity.
Build your matrix around critical daily operations:
| Role | Primary Tasks | Emergency Coverage Skills | Time to Basic Competency |
|---|---|---|---|
| Front Desk | Check-in, phones, scheduling | Insurance verification basics, payment posting | 5-7 days |
| Clinical Assistant | Patient prep, therapy support, equipment | Basic scheduling, check-out process | 3-4 days |
| Office Manager | Operations, reporting, staff oversight | Full front desk, basic billing | Already trained |
| Billing Specialist | Claims, posting, denials | Front desk phones, eligibility checks | 2-3 days |
The key is "good enough" competency for emergency coverage, not mastery. Your clinical assistant doesn't need to handle complex insurance appeals—just basic eligibility verification. Your billing specialist doesn't need scheduling expertise, just the ability to book simple follow-ups.
Document these skills in one-page reference sheets, not lengthy manuals. Include screenshots, specific phrases, and common scenarios. Test competency monthly during slow periods with basic mock situations.
Protecting revenue during transition periods
Staffing transitions cost more than replacement hiring fees. The real expense comes from lost appointments, scheduling errors, overtime, and patient defection during the chaos. Most clinics lose somewhere between 15-25% of monthly revenue during significant staffing changes.
Week 1-2: Immediate stabilization
-
Lock your schedule template. No changes, no exceptions.
-
Pull your strongest performer into pure scheduling oversight.
-
Their only job
prevent double-bookings, gaps, and patient conflicts.
Set up temporary overflow systems. Route new patient calls to voicemail with same-day callback promises. Move follow-up bookings online only. Push non-urgent tasks like records requests to next week. You're buying time, not solving everything.
Week 3-4: Selective automation
-
Deploy automated confirmations for every appointment—text and email.
-
Set up waitlist notifications for last-minute openings.
-
Create auto-responses for common insurance questions.
These automations alone can reduce call volume by roughly 35%, giving your skeleton crew actual breathing room.
Week 5+: Strategic rebuilding
Only now do you start optimizing. Look at which scheduling patterns survived the crisis—those are your most resilient workflows. Figure out which tasks genuinely require experienced staff versus what can be systematized.
Then hire for specialized roles rather than generalists. A dedicated insurance verifier at $22/hour usually beats a $28/hour "do everything" coordinator who burns out and quits in three months.
When to abandon traditional hiring completely
Some clinics are better off never hiring traditional full-time staff again. That sounds extreme until you look at the numbers. Between benefits, payroll taxes, PTO coverage, and training, a $20/hour employee actually costs closer to $31/hour. Add turnover and you're pushing $35/hour for unstable coverage.
Virtual assistant services: $8-12/hour for scheduling, reminder calls, and basic admin. Quality varies, but for routine tasks, even 70% effectiveness beats 0% coverage during staff absence.
Shared staffing pools: Partner with two or three nearby clinics to share specialized roles. One billing specialist across three practices. One marketing coordinator handling all locations. Costs split, expertise consolidated.
Task-specific contractors: Instead of one person doing eight tasks adequately, hire people doing one task well. Your insurance verifier works 10 hours weekly. Your recall specialist handles only rebooking. Your scheduler only schedules.
This fragmented approach seems messy but it creates real resilience. Losing one contractor disrupts maybe 12% of operations, not everything. You can replace a single-task contractor in days, not months.
Technology bridges that work (and those that don't)
The instinct during staffing crises is to throw software at the problem. But most clinic platforms make operations worse during transitions. Complex EMR systems and comprehensive practice management suites require training time you don't have.
Simple scheduling overlays: Tools that sit on top of your existing system but simplify the interface. New staff can book appointments without learning complex software from scratch. One practice reduced scheduling training from two weeks to two days with a basic Google Calendar integration.
SMS-first patient communication: Forget patient portals during a crisis. Text confirmations, rescheduling links, and basic question handling. Response rates are around 94% versus 31% for email. Staff efficiency improves significantly when they're managing text threads instead of playing phone tag.
Voice-to-task automation: Basic AI transcription that converts voicemails into task lists. "Patient needs Thursday afternoon appointment" becomes a scheduling task. "Insurance question about coverage" routes to billing. Cuts message processing time substantially.
The filter is simple: if it takes more than 30 minutes to train someone on it, it's too complex for crisis deployment.
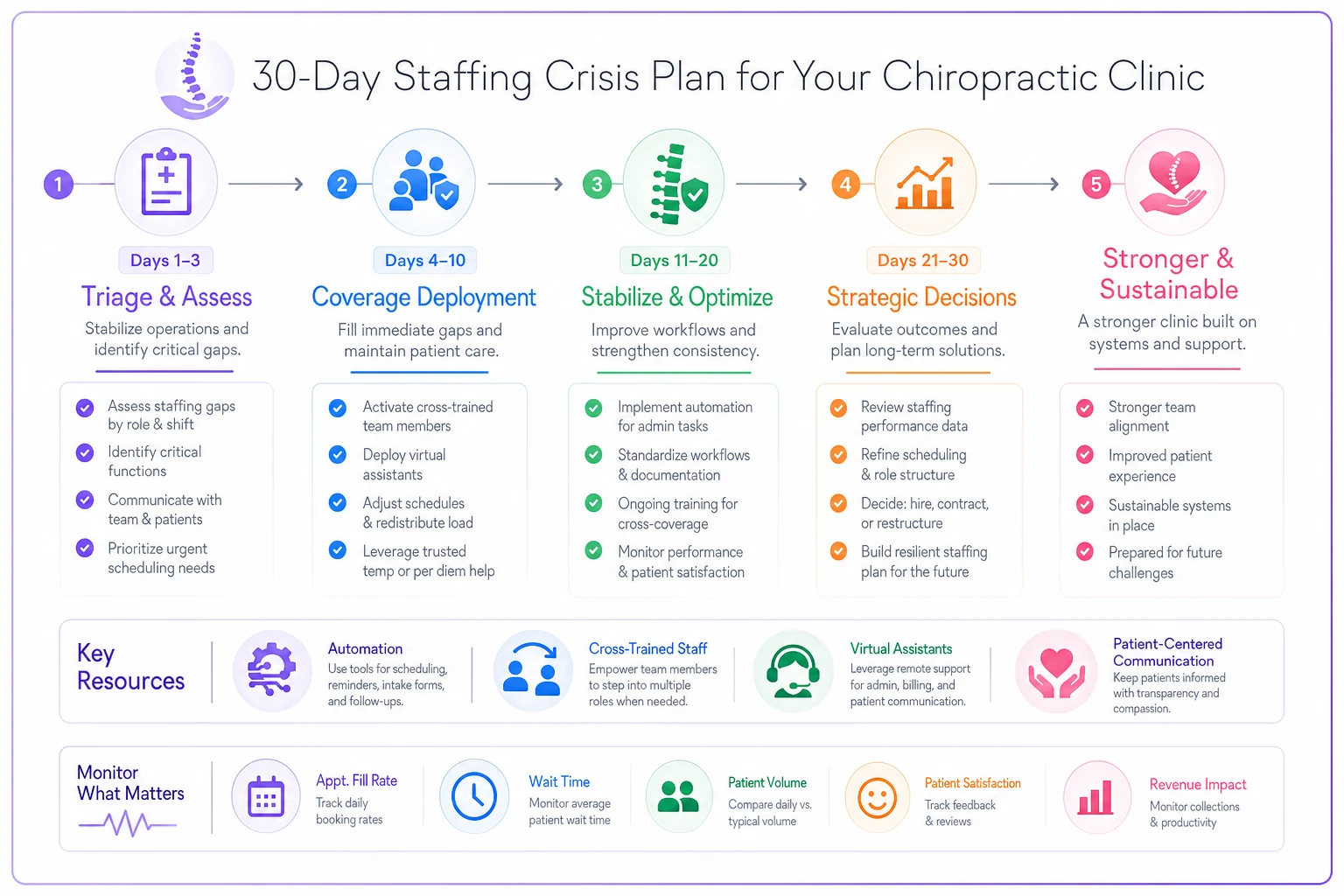
Building your 30-day staffing crisis plan
Staffing crises will happen. The question is whether you scramble reactively or execute a plan you already built. Here's a framework that's kept clinics operational during staffing chaos:
Days 1-3: Immediate triage
-
Cancel all non-essential meetings
-
Pull office manager to full-time scheduling oversight
-
Activate overflow voicemail systems
-
Notify patients of potential delays via mass text
-
Lock schedule template to prevent changes
Days 4-10: Coverage deployment
-
Activate cross-trained staff for critical tasks
-
Deploy temporary automation for confirmations
-
Hire virtual assistant for phone coverage
-
Begin daily chair utilization tracking
-
Create simplified reference sheets for complex tasks
Days 11-20: Stabilization
-
Assess which workflows are holding
-
Identify revenue leakage points
-
Begin selective task outsourcing
-
Interview temporary contractors
-
Implement basic performance metrics
Days 21-30: Strategic decisions
-
Evaluate permanent structural changes
-
Decide on hybrid versus traditional staffing
-
Implement tested automation permanently
-
Begin selective hiring if needed
-
Document what you learned
Below is a visual workflow of the 30-day plan.
The clinics that survive staffing crises aren't the ones with the best hiring processes—they're the ones with the best contingency systems already in place.
Turning staffing volatility into competitive advantage
While competitors panic about unfilled positions, you can build operations that assume instability. Not accepting mediocrity—building systems that maintain service quality regardless of who shows up Monday morning.
Map every critical task in your clinic and identify three ways to complete it. Primary method under normal staffing. Secondary method in coverage mode. Tertiary method during full crisis. Scheduling might normally run through your experienced coordinator, shift to cross-trained clinical staff during gaps, and fall back to a virtual assistant in a real emergency.
Document contingencies in one-page flowcharts, not lengthy manuals. When things go sideways, nobody's reading procedure guides. They need simple decision trees: "If scheduling coordinator is out more than two days, activate virtual assistant backup."
There's also an underappreciated side effect: clinics with solid contingency plans tend to have better staff retention. People stay longer when they know coverage systems exist. They take vacations without guilt. They don't burn out covering for missing colleagues indefinitely. Having a Plan B actually stabilizes Plan A.
Connecting systematic hiring to crisis prevention
The current labor market isn't turning around quickly. Layoffs in manufacturing are at levels not seen since the financial crisis and COVID, which is creating unusual labor market dynamics across industries. Clinics that build systematic hiring and competency frameworks can prevent most staffing crises before they start—by shifting from reactive hiring to actual talent pipeline development.
That means maintaining warm relationships with potential hires before you need them. Building competency faster through structured onboarding. Creating growth paths that reduce turnover. And accepting that perfect staffing is a myth, then building operations that work anyway.
The clinics doing well right now aren't waiting for the ideal candidate. They're building systems that turn average people into effective operators through smart process design, selective automation, and realistic expectations.
Your next staffing crisis is coming—probably sooner than you'd like. The question isn't whether you'll face gaps, but whether those gaps will cripple operations or just slow them temporarily. Build your contingencies now, while you still have time and calm to think. Because when your office manager gives notice next Monday, it's already too late to start planning.
Ready to streamline your chiropractic clinic operations?
Join 1,200+ clinics using Spinesly to save time, reduce scheduling errors, and improve patient care experiences.